Dental
Injuries to the mouth and/or teeth can result from a fall on the face or a direct blow, such as a punch.
A blow under the jaw can result in bitten lips or tongue. Such injuries can be associated with severe bleeding, which can be a risk to the patient’s airway. If a tooth is knocked out in a collision or fall, the correct first aid may save the tooth.
Swelling in or around the mouth can be associated with an injury or severe allergic reaction. This can cause obstruction to the throat and upper airway for which prompt medical assessment and treatment are required.
Symptoms and signs – Not all may be present
- bleeding from the mouth, lips, tongue or tooth socket
- pain around or in the mouth following an injury
- a broken or displaced tooth
- swelling in the mouth or around the jaw
How you can help
1. Assess the patient and the injury
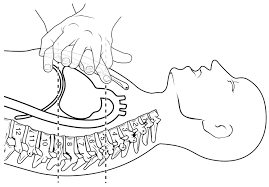
- Check that the patient’s airway is clear. If there is any risk of blood going down the throat or of increased swelling of the mouth, tongue or throat, turn the patient on the side in a supported position.
- If the bleeding is only slow or moderate and there appears to be no breathing difficulty, assist the patient into the position of greatest comfort – generally sitting or half-sitting – and check the site of any bleeding.
2. Control any bleeding
- Apply firm pressure to any bleeding wound or tooth socket. Fold a sterile dressing or clean tissue into a pad and ask the patient to hold it firmly on the bleeding site for at least 10 minutes.
- If the bleeding is coming from a cut lip, advise the patient to hold the injured area firmly between the folds of a moist tissue or dressing.

If a tooth has been knocked out:
- Handle the displaced tooth by the crown and not the root.
- Ask the patient to suck it clean and then try to replace the tooth in the original position in the socket to keep the root alive. A small piece of folded aluminium foil may be used as a splint to fix the tooth in place until a dentist is available. A dentist should see the patient within 30 to 60 minutes if the tooth is to be saved.
- Wrap the foil splint over at least one tooth on each side of the replaced tooth. Ask the patient to bite down firmly on the splint to keep the tooth root in contact with the tissues of the jaw.
- If the patient cannot assist with replacement of the tooth in the socket, try to keep the tooth moist and clean. If the patient is fully alert, ask the patient to carry the tooth in the mouth between the lower front teeth and lip where it will be bathed in saliva.
- If the patient is unconscious place the tooth in a clean container with a little milk.
If the bleeding follows the extraction of a tooth by a dental surgeon:
- Ask the patient to bite down firmly over a pad that covers the tooth socket.
- Continue to maintain pressure over the pad for at least 10 to 20 minutes to allow a new clot to form.
Obtain medical or dental advice
- If the injury involves a tooth or the jaw, arrange prompt transport to a dentist or dental hospital. If fully alert, the patient may be transported in a private vehicle.
- If there is serious bleeding or swelling of the mouth or throat, the patient needs to see a doctor.

First aid -Cut and wounds
Introduction:
Cuts are open wounds through the skin. Normally the skin is under slight, constant tension as it covers the body. A cut is a forceful injury to the skin. Many people accidentally cut themselves with household or work items, yard tools, or when operating machinery. Children often are cut during play and sports activities, or from falls while riding wheeled toys, such as bikes, scooters, or skateboards. Most cuts are minor and home treatment is usually all that is needed.
Cuts can be caused by:
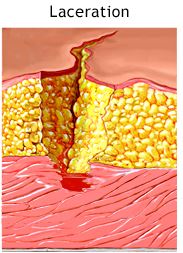
- Blunt objects that tear or crush the skin (lacerations). These cuts are more common over bony areas, such as a finger, hand, knee, or foot, but they can occur anywhere on the body. Blunt object injuries usually cause more swelling and tissue damage and leave jagged edges, so problems with healing may occur.
- Sharp-edged pointed objects pressing into and slicing the skin tissue (incised wounds). Sharp object injuries are more likely to cut deeper and damage underlying tissue.
- Sharp-edged objects piercing the skin tissue (stab or puncture wounds).
- A combination of blunt and sharp objects that tear, crush, and slice the skin tissue.


Symptoms:
Symptoms include:
- Problems with function or feeling below the wound site
Infection may occur with some cuts and puncture wounds. The following are more likely to become infected:
- Wounds that are not promptly treated
Types of cuts:
Some types of cuts are more serious and need medical evaluation and treatment. These more serious cuts include:
- Cuts that open with movement of the body area, such as a cut over a joint. A cut over a joint may take a long time to heal because of the movement of the wound edges.
- Cuts that may scar and affect the appearance or function of a body area. A cut on an eyelid or lip which doesn’t heal well may interfere with function or leave a noticeable scar.
- Cuts that remove all of the layers of the skin (avulsion injuries), such as slicing off the tip of a finger. An avulsion injury may take a long time to heal.
- Cuts from an animal or human bite. Infection is more likely with a bite injury.

- Cuts that have damage to underlying tissues. Injuries to nerves, tendons, or joints are more common with cuts on the hands or feet. Slight swelling, bruising, and tenderness around a cut, bite, scrape, or puncture wound is normal. Swelling or bruising that begins within 30 minutes of the injury often means there is a large amount of bleeding or that damage to deeper tissues is present.
- Cuts over a possible broken bone. Bacteria can get into a cut over a broken bone and infect the bone.
- Cuts caused by a crushing injury. With this type of injury, the cut may have occurred when the skin split open from the force of the injury. The force of the injury may also damage underlying tissues and blood vessels. Crush injuries have a high risk of infection.
- Cuts with a known or suspected object, such as glass or wood, in the wound.
Injury to the skin may also break small blood vessels under the skin and cause more swelling and bruising than you would expect.
When you have a cut:
- Stop the bleeding with direct pressure to the wound.
- Determine if other tissues, such as blood vessels, nerves, tendons, ligaments, joints, bones, or internal organs, have been injured.
- Determine if treatment by a doctor, such as stitches, staples, or skin adhesives, is needed.
- Clean the wound and remove any dirt or debris to prevent infections, both bacterial skin infections and tetanus (“lockjaw”).
- Determine whether you need a tetanus shot.
Cuts to the head or face may appear worse than they are and bleed a lot because of the good blood supply to this area. Controlling the bleeding will allow you to determine the seriousness of the injury.
FOR MINOR CUTS:
- Wash your hands with soap or antibacterial cleanser to prevent infection.
- Then, wash the cut thoroughly with mild soap and water.
- Use direct pressure to stop the bleeding.
- Apply antibacterial ointment and a clean bandage that will not stick to the wound.

FOR MINOR PUNCTURES:
- Wash your hands with soap or antibacterial cleanser to prevent infection.
- Rinse the puncture for 5 minutes under running water. Then wash with soap.
- Look (but do not poke around) for objects inside the wound. If found, don’t remove it. Go to your emergency or urgent care center.
- If you can’t see anything inside the wound, but a piece of the object that caused the injury is missing, also seek medical attention.
- Apply antibacterial ointment and a clean bandage that will not stick to the wound.
If emergency treatment is not needed, bleeding can usually be stopped by applying steady, direct pressure and elevating the wound. The following steps will protect the skin wound and protect you from exposure to another person’s blood.
 Stop the bleeding
Stop the bleeding
- Have the injured person lie down and elevate the site that is bleeding.
- Remove any visible objects in the wound that are easy to remove. Control the bleeding before trying to clean the wound.
- Remove or cut clothing from around the wound. Remove any jewelry from the general area of the wound so if the area swells, the jewelry will not affect blood flow.
- Apply steady, direct pressure and elevate the area for a full 15 minutes. Use a clock—15 minutes can seem like a long time. Resist the urge to peek after a few minutes to see whether bleeding has stopped. If blood soaks through the cloth, apply another one without lifting the first. If there is an object in the wound, apply pressure around the object, not directly over it.
- If moderate to severe bleeding has not slowed or stopped, continue direct pressure while getting help. Do not use a tourniquet to stop the bleeding. Do all you can to keep the wound clean and avoid further injury to the area.
- Mild bleeding usually stops on its own or slows to an ooze or trickle after 15 minutes of pressure. It may ooze or trickle for up to 45 minutes.

Clean the wound
Clean the wound as soon as possible to reduce the chance of infection, scarring, and tattooing of the skin from dirt left in the wound.
- Remove large pieces of dirt or other debris from the wound with cleaned tweezers. Do not push the tweezers deeply into the wound.
- Wash the wound for 5 minutes with large amounts of cool water and soap (mild dish washing soap, such as Ivory, works well). Some nonprescription products are available for wound cleaning that numb the area so that cleaning doesn’t hurt as much. Be sure to read the product label for correct use.
- Don’t use rubbing alcohol, hydrogen peroxide, iodine, or Mercurochrome, which can harm the tissue and slow healing.
Consider applying a bandage
Most cuts heal well and may not need a bandage. You may need to protect the cut from dirt and irritation. Be sure to clean the cut thoroughly before bandaging it to reduce the risk of infection occurring under the bandage.
- Select the bandage carefully. There are many products available. Liquid skin bandages and moisture-enhancing bandages are available with other first aid products. Before you buy or use one, be sure to read the label carefully, and follow the label’s instructions when you apply the bandage.
- If you use a cloth-like bandage, apply a clean bandage when it gets wet or soiled to further help prevent infection. If a bandage is stuck to a scab, soak it in warm water to soften the scab and make the bandage easier to remove. If available, use a nonstick dressing. There are many bandage products available. Be sure to read the product label for correct use.
- Watch for signs of infection. If you have an infection under a bandage, a visit to your doctor may be needed.
- An antibiotic ointment, such as polymyxin B sulfate (for example, Polysporin) or bacitracin, will keep the bandage from sticking to the wound. Apply the ointment lightly to the wound. Antibiotic ointments have not been shown to improve healing. Be sure to read the product label about skin sensitivity. If you have a skin rash or itching under the bandage, stop using the ointment. The rash may be caused by an allergic reaction to the ointment.
- Use an adhesive strip to hold the edges of a wound together. Always put an adhesive strip across a wound to hold the edges together, not lengthwise. You can make a butterfly bandage at home or purchase one to help hold the skin edges together.

DO NOT:
- Do NOT assume that a minor wound is clean because you can’t see dirt or debris inside. Always wash it.
- Do NOT breathe on an open wound.
- Do NOT try to clean a major wound, especially after the bleeding is under control.
- Do NOT remove a long or deeply stuck object. Seek medical attention.
- Do NOT push or pick debris from a wound. Seek medical attention.
- Do NOT push body parts back in. Cover them with clean material until medical help arrives.
First aid for cut and scrapes