Overview:
Frostbite occurs when tissues freeze. This condition happens when you are exposed to temperatures below the freezing point of skin. Hypothermia is the condition of developing an abnormally low body temperature. Frostbite and hypothermia are both cold-related medical emergencies.
Although frostbite used to be a military problem, it is now a civilian one as well. The nose, cheeks, ears, fingers, and toes are most commonly affected. Everyone is susceptible, even people who have been living in cold climates for most of their lives. Some groups of people at greatest risk for frostbite and hypothermia include those:
- who spend a great deal of time outdoors, such as the homeless, hikers, hunters, etc.;
- under the influence of alcohol;
- who are elderly without adequate heating, food, and shelter;
- who are exhausted or excessively dehydrated;
- who are mentally ill.
When exposed to very cold temperatures, skin and underlying tissues may freeze, resulting in frostbite. The areas most likely to be affected by frostbite are your fingers toes, nose, ears, cheeks and chin.
If your skin pales or turns red and is very cold, hard or waxy looking, you may have frostbite. You may also experience a prickling feeling or numbness. With severe or deep frostbite, you may experience blistering and pain.
You can treat very mild frostbite (frost nip) with first-aid measures.All other frostbite requires medical attention.
Definition:
Frostbite is damage to the skin and underlying tissues caused by extreme cold. Frostbite is the most common freezing injury.
Alternative Names:
Cold exposure – arms or legs
Causes:
In conditions of prolonged cold exposure, the body sends signals to the blood vessels in the arms and legs telling them to constrict (narrow). By slowing blood flow to the skin, the body is able to send more blood to the vital organs, supplying them with critical nutrients, while also preventing a further decrease in internal body temperature by exposing less blood to the outside cold.
Frostbite occurs when the skin and body tissues are exposed to cold temperature for a long period of time.
You are more likely to develop frostbite if you:
- Take medicines called beta-blockers
- Have poor blood supply to the legs
- Smoke
- Have diabetes
- Have Raynaud’s phenomenon
Frostbite is caused by two different means: cell death at the time of exposure and further cell deterioration and death because of a lack of oxygen.
- In the first, ice crystals form in the space outside of the cells. Water is lost from the cell’s interior, and dehydration promotes the destruction of the cell.
- In the second, the damaged lining of the blood vessels is the main culprit. As blood flow returns to the extremities upon rewarming, it finds that the blood vessels themselves are injured, also by the cold. The vessel walls become permeable and blood leaks out into the tissues. Blood flow is impeded and turbulent and small clots form in the smallest vessels of the extremities. Because of these blood flow problems, complicated interactions occur, leading to inflammation that causes further tissue damage. This injury is the primary determinant of the amount of tissue damage that occurs in the end.
- It is rare for the inside of the cells themselves to be frozen. This phenomenon is only seen in very rapid freezing injuries, such as those produced by frozen metals.
Symptoms:
Symptoms of frostbite include:
- Pins and needles feeling, followed by numbness.
- Hard, pale, and cold skin that has been exposed to the cold for too long.
- Aching, throbbing or lack of feeling in the affected area.
- Red and extremely painful skin and muscle as the area thaws.
Very severe frostbite may cause:
- Blisters.
- Gangrene (blackened, dead tissue).
- Damage to tendons, muscles, nerves, and bone.
Frostbite may affect any part of the body. The hands, feet, nose, and ears are the places most prone to the problem.
- If the frostbite did not affect your blood vessels, a complete recovery is possible.
- If the frostbite affected the blood vessels, the damage is permanent. Gangrene may occur. This may require removal of the affected body part (amputation).
Types of frostbite:
A variety of frostbite classification systems have been proposed. The easiest to understand, and perhaps the one that gives the best clues to outcome, divides frostbite into two main categories:
1) superficial and
2) deep.
- In superficial frostbite, you may experience burning, numbness, tingling, itching, or cold sensations in the affected areas. The regions appear white and frozen, but if you press on them, they retain some resistance.
- In deep frostbite, there is an initial decrease in sensation that is eventually completely lost. Swelling and blood-filled blisters are noted over white or yellowish skin that looks waxy and turns a purplish blue as it rewarms. The area is hard, has no resistance when pressed on, and may even appear blackened and dead.
- The affected person will experience significant pain as the areas are rewarmed and blood flow reestablished. A dull continuous ache transforms into a throbbing sensation in 2 to 3 days. This may last weeks to months until final tissue separation is complete.
- At first the areas may appear deceptively healthy. Most people do not arrive at the doctor with frozen, dead tissue. Only time can reveal the final amount of tissue damage.
There are milder conditions related to frostbite, including frost nip, chilblains, and trench foot.
- Frost nip refers to the development of tingling sensations (parenthesizes) that occur due to cold exposure. They disappear upon rewarming without any tissue damage.
- Chilblain (or pernio) refers to a localized area of tissue inflammation that appears as swollen and reddish or purple. These develop in response to repeated exposure to damp, cold conditions above the freezing point. Chilblains may itch or be painful.
- Trench foot was described in World War I as a result of repeated exposure to dampness and cold and exacerbated by tight boots. The affected feet are reddened, swollen, painful or numb, and may be covered with bleeding blisters. This condition is still observed in some homeless persons today.
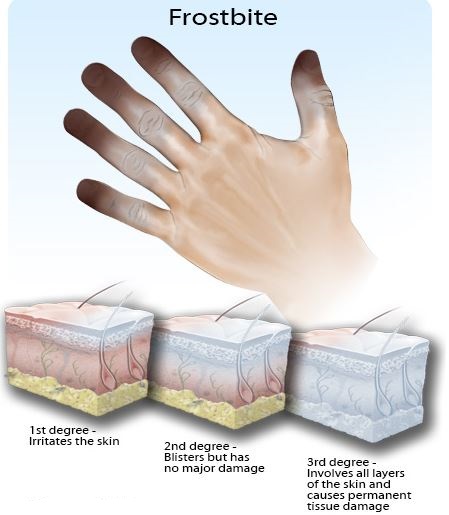
Stages of frostbite:
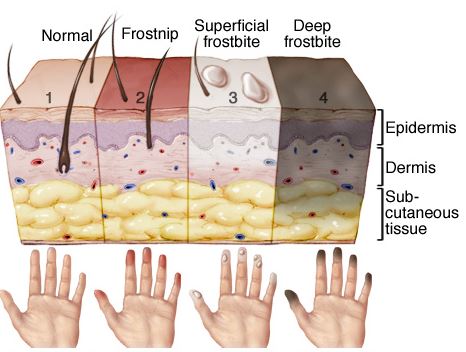
Skin without cold damage is normal:
(1). Frostnip.
(2) is mild frostbite that irritates the skin, causing redness, prickling and a cold feeling followed by numbness. Frostnip doesn’t permanently damage the skin and can be treated with first-aid measures. With superficial frostbit.
(3), your skin feels warm, a sign of serious skin involvement. A fluid-filled blister may appear 24 to 36 hours after rewarming the skin. With deep frostbite.
(4), you may experience numbness. Joints or muscles may no longer work. Large blisters form 24 to 48 hours after rewarming. Afterward, the area turns black and hard as the tissue dies.
First Aid:
A person with frostbite on the arms or legs may also have hypothermia (lowered body temperature). Check for hypothermia and treat those symptoms first.
Take the following steps if you think someone might have frostbite:
- Shelter the person from the cold and move him or her to a warmer place. Remove any tight jewelry and wet clothes. Look for signs of hypothermia (lowered body temperature) and treat that condition first.
- If you can get quick medical help, it is best to wrap the damaged areas in sterile dressings. Remember to separate affected fingers and toes. Transport the person to an emergency department for further care.
- If medical help is not nearby, you may give the person rewarming first aid. Soak the affected areas in warm (never hot) water — for 20 to 30 minutes. For ears, nose, and cheeks, apply warm cloths repeatedly. The recommended water temperature is 104 to 108 degrees Fahrenheit. Keep circulating the water to aid the warming process. Severe burning pain, swelling, and color changes may occur during warming. Warming is complete when the skin is soft and feeling returns.
- Apply dry, sterile dressings to the frostbitten areas. Put dressings between frostbitten fingers or toes to keep them separated.
- Move thawed areas as little as possible.
- Refreezing of thawed extremities can cause more severe damage. Prevent refreezing by wrapping the thawed areas and keeping the person warm. If protection from refreezing cannot be guaranteed, it may be better to delay the initial rewarming process until a warm, safe location is reached.
- If the frostbite is severe, give the person warm drinks to replace lost fluids.
When to Contact a Medical Professional:
Call your doctor or nurse if:
- You had severe frostbite.
- Normal feeling and color do not return promptly after home treatment for mild frostbite.
- Frostbite has occurred recently and new symptoms develop, such as fever, general ill-feeling, skin discoloration, or drainage from the affected body part.
Self Care at home:
- First, call for help.
- Keep the affected body part elevated in order to reduce swelling.
- Move to a warm area to prevent further heat loss.
- Note that many people with frostbite may be experiencing hypothermia. Saving their lives is more important than preserving a finger or foot.
- Do not walk on frostbitten toes or feet if at all possible.
- Remove all wet clothing and constrictive jewelry because they may further block blood flow.
- Give the person warm, nonalcoholic, non caffeinated fluids to drink.
- Apply a dry, sterile bandage, place cotton between any involved fingers or toes (to prevent rubbing), and take the person to a medical facility as soon as possible.
- Do not rub the frozen area with snow (or anything else). The friction created by this technique will only cause further tissue damage.
Dos:
- DO keep the water moving a little. It helps keep the warmest water next to the injury.
- DO be very gentle with the damaged tissue.
- DO handle with care.
- DO keep the injured area at heart level or above.
- DO consider taking a vasodilator (medicine that opens up the blood-vessel flow). Some blood-pressure medicines help if you’re already on them. Aspirin may help.
- DO keep absorbent padding, such as gauze or cotton, between injured fingers or toes.
- DO cover the wound with a light dressing or leave it open to the air.
- DO Get to a warm room or environment immediately.
Do Not:![]()
- Do NOT thaw out a frostbitten area if it cannot be kept thawed. Refreezing may make tissue damage even worse.
- Do NOT use direct dry heat (such as a radiator, campfire, heating pad, or hair dryer) to thaw the frostbitten areas. Direct heat can burn the tissues that are already damaged.
- Do NOT rub or massage the affected area.
- Do NOT disturb blisters on frostbitten skin.
- Do NOT smoke or drink alcoholic beverages during recovery as both can interfere with blood circulation.
- Don’t use restrictive dressings.
- Don’t walk, stand, or put pressure on the injured area.
Frostbite Prevention:
The first step in preventing frostbite is knowing whether you are at increased risk for the injury.
- Most cases of frostbite are seen in alcoholics, people with psychiatric illness, victims of car accidents or car breakdowns in bad weather, and cases of recreational drug misuse.
- All of these conditions share the problem of cold exposure and either the unwillingness or inability of a person to remove himself or herself from this threat.
- Tobacco smokers and people with diseases of the blood vessels (such as those with diabetes) also are at increased risk because they have an already decreased amount of blood flow to their arms and legs.
- Homelessness, fatigue, dehydration, improper clothing, and high altitude are additional risk factors.
Although people don’t always know or acknowledge these dangers, many of the dangers can be reduced or prevented.
- Dress for the weather.
- Layers are best, and mittens are better than gloves (keeps your warm fingers together while warming each other).
- Wear two pairs of socks with the inner layer made of synthetic fiber, such as polypropylene, to wick water away from the skin and the outer layer made of wool for increased insulation.
- Shoes should be waterproof.
- Cover your head, face, nose, and ears at all times.
- Clothes should fit loosely to avoid a decrease in blood flow to the arms and legs.
- Always travel with a friend in case help is needed.
- Avoid smoking and alcohol.
- The very old, very young, those who are not in good physical condition, and people with diabetes and anyone with vessel disease should take extra precautions.
- Be especially wary of wet and windy conditions. The “feels like” temperature (windchill) is actually much lower than the stated air temperature.